

Breast cancer treatment is improving all the time, but that’s not enough: we need to diagnose the disease more accurately and target treatments more effectively. With the arrival of new targeted therapies for patients with low or very low expression of the HER2 receptor, there is a clinical imperative to refine and make more reliable the diagnosis of this biomarker, which has become central to therapeutic decisions.
This demand for precision is matched by another upheaval: the rise of digital pathology and artificial intelligence algorithms capable of assisting pathologists in the detailed assessment of HER2. While these technologies are promising, their deployment in routine clinical practice still raises crucial questions: reliability, robustness, interpretability and acceptability to professionals.
It is at this juncture, between therapeutic progress and technological innovation, that a strong need is emerging on the ground: to ensure that the AI tools now available meet clinical requirements and are effectively integrated into medical practices.
To meet this challenge, a number of players are mobilising, drawing on their complementary strengths and their shared commitment to innovation for the benefit of patients:
Together, these partners are launching AI for Her, a call for solutions to identify, test and develop the best AI technologies applied to digital pathology in breast cancer.
The aim is clear : to enable every patient to benefit from the most appropriate therapy, as early as possible.

AI for Her
The pioneers of the greatest scientific discoveries and advances did not set out alone. Positive competition, team spirit and collective ambition in the service of a better tomorrow have been extraordinary drivers of development.
AI for Her aims to be an unprecedented challenge and a collective cooperative movement bringing together the worlds of technology and science to improve the care and treatment of breast cancer patients and help medical staff by bringing ever greater precision, objectivity and reproducibility to their diagnoses.
For a period of 6 to 9 months, anatomopathologists and start-ups developing an artificial intelligence solution capable of scoring HER2 (one of the Human Epidermal growth factor Receptor typologies playing a key role in breast cancer) at low and ultra-low expression levels, will be combining their expertise and focusing their energies on evaluating the performance and use of AI algorithms.
AI for Her is the very first challenge to enable AI algorithms to be evaluated in real life, at the heart of the hospital, thanks to the organisation of an entire cancer centre.
For methodological reasons, the study was divided into two sub-studies.
Study A: assessing the performance of all the solutions
Comparative evaluation of the performance of several artificial intelligence tools for low and ultra-low expression HER2 scoring in breast cancer. No calibration is planned for this study of the entire cohort. At the end of this study, the two algorithms judged to perform best according to the defined evaluation criteria will be selected for Study B.
Study B: assessing the impact of the two selected solutions
To assess the impact of artificial intelligence on the diagnostic performance of pathologists in scoring low-expression HER2 in breast cancer. A calibration is planned for this study. 4 pathologists, divided into two groups (non-experienced and experienced) will individually evaluate all the slides from the ICO cohort without AI, and then with each AI selected in study A.
The study involved a retrospective global cohort of breast cancer cases consisting of :
The performance of each solution (algorithm) will be assessed against two gold standards representative of current practices: (1) slide scoring by Labcorp*, and (2) slide scoring by experts from GEFPICS**.
Each algorithm will be compared with the two gold standards with the aim of comparing with current practices and not discriminating between the best gold standard.
The performance of the algorithms will be assessed mainly on the basis of the following quantitative and semi-qualitative criteria :
The performance of each solution will be assessed in accordance with the scoring grid below :
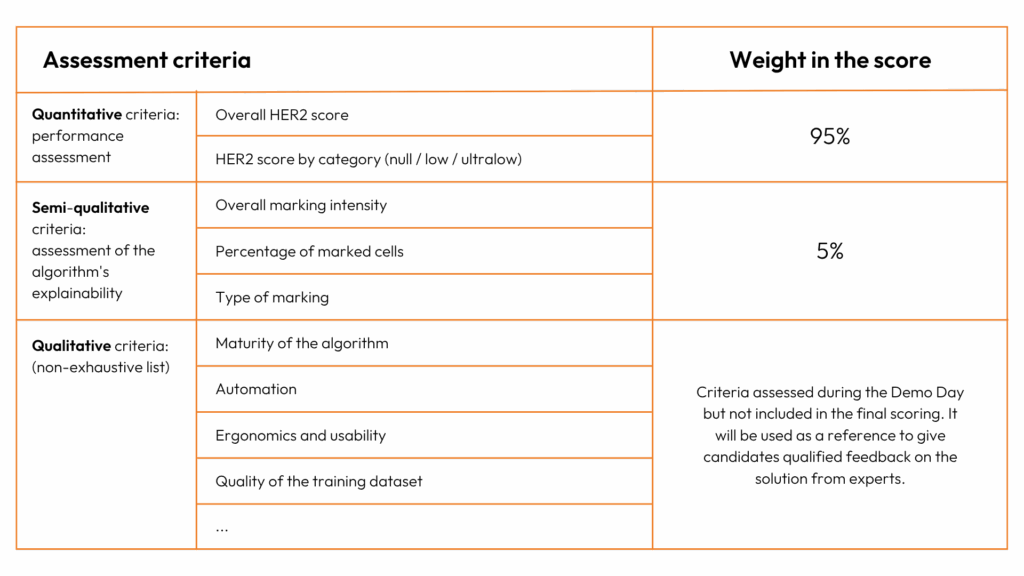
It should be noted that, in addition to the quantitative and semi-qualitative criteria, the project’s scientific committee will note, for each solution, qualitative information relating to the robustness, ergonomics and maturity of the solution, which will constitute, for each candidate start-up, concrete feedback from the experts. This qualitative information will nonetheless not be taken into account in the performance evaluation score.

*LABCORP: Laboratory Corporation of America Holdings is one of the world’s leading providers of medical laboratory analysis and diagnostic services. Present in more than 100 countries, the company offers a wide range of laboratory tests, from routine analyses to specialist examinations in genetics, oncology, infectious diseases and reproductive health.
Thanks to a strong capacity for innovation and the integration of the latest scientific advances, Labcorp supports healthcare professionals in the prevention, diagnosis and monitoring of pathologies, while contributing to clinical research. Its objective: to improve medical decisions and care pathways for a better state of health for patients throughout the world.
**GEFPICS: The Groupe d’Etude des Facteurs Pronostiques Immunohistochimiques dans le Cancer du Sein (Group for the Study of Immunohistochemical Prognostic Factors in Breast Cancer) is a French scientific group made up of experts in anatomopathology, oncology and medical biology, whose main objective is to standardise and improve the evaluation of immunohistochemical markers in breast cancer, and in particular: to establish technical and interpretative recommendations for the immunohistochemical analysis of biomarkers, to harmonise diagnostic practices, and to help improve the quality of diagnosis.
(1) Having developed an algorithm for scoring low and ultra-low HER2 expression in breast cancer.
(2) This algorithm must be CE marked (or equivalent), in the process of being marked or at a level of maturity that allows it to apply for marking in the near future
(3) Having a functional algorithm with the IHC slides used in the study: staining with the Roche Ventana Automated Benchmark Ultra and Roche Ac 4B5; Scanning with the Leica Aperio GT450 and 3D HISTECH scanner.
(4) The results of the algorithm must be provided in a report in a usable format (csv, xls, etc.) enabling each slide and its associated performance criteria to be identified, as well as the average processing time per slide and the technical failure rate (number of slides on which the AI was unable to reach a decision in relation to the total number of slides assessed.
(5) Being able to provide, within the allotted time and with the results, the server logs to ensure that the results are autonomous.
Applications must be sent via the dedicated platform. The application must include all the documents requested:
Projects must be submitted during the opening period of the call for projects and will then be collected and processed on the closing date of this period.
Applications will be analysed on the basis of the above-mentioned eligibility criteria and the completeness of the application. Applicants who meet these two conditions will continue the selection process and will then be able to demonstrate their solution at a Startups Demo Day in front of three GEFPICS experts, the industrial partner and all the ICO healthcare professionals involved in the project (pathologist, oncologist and AI expert). This Startups Demo Day is a unique opportunity to showcase your technology to those working in the field.
It has already been agreed that this Demo Day will enable GEFPCIS experts to evaluate the qualitative criteria of the algorithm that will be used for the final performance rating.
At the end of the demonstration, the members of the jury will decide which technological solutions will be selected to take part in the study on the basis of compliance with the eligibility criteria for the solution and assessment of the qualitative criteria..
Participating candidates will have unprecedented access to all the expertise and resources of the Institut Cancérologique de l’Ouest to test, debug and optimise their solution using real-life data. There is no financial compensation, but participants will have access to various prizes depending on their ranking in the AI for Her challenge :

NB. With the exception of the solutions ranked first and second, the results published will be anonymous. Each participant will be informed anonymously of his or her performance ranking in relation to the other participants.
***DMH: The Digital Medical Hub is a key player in digital innovation in healthcare, supporting projects from clinical trials through to market access, integrating the associated product and regulatory strategy. For AI for Her, the Digital Medical Hub is responsible for the methodological aspects of the study (drafting and registration of the protocol), as well as assisting the winner with an early meeting with the HAS.
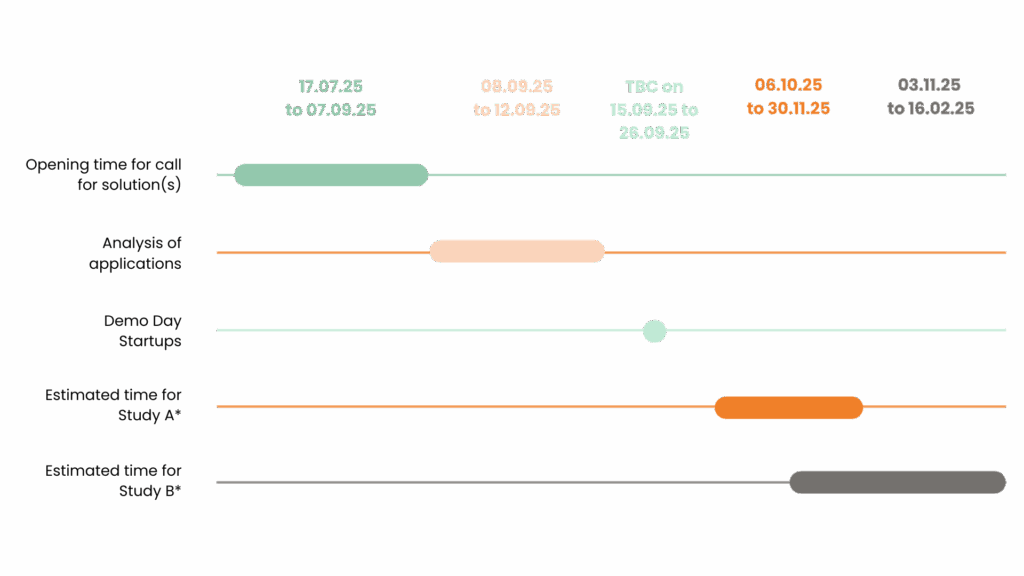
*The launch of studies A and B is subject to contractual agreement with all stakeholders.
For Study A, the timeframe indicated is that of the complete study including statistical analysis of the results. The duration of the scoring of the algorithms is to be determined, but will be spread over a shorter period (a few days).
For study B, the timeframe indicated concerns the three scoring stages (without AI, with AI A, with AI B), each of which will be spread over a few days, with a month’s wash-out planned between each stage to ensure the objectivity of the results. The timeline could extend to the end of February, including the analysis of the final results.

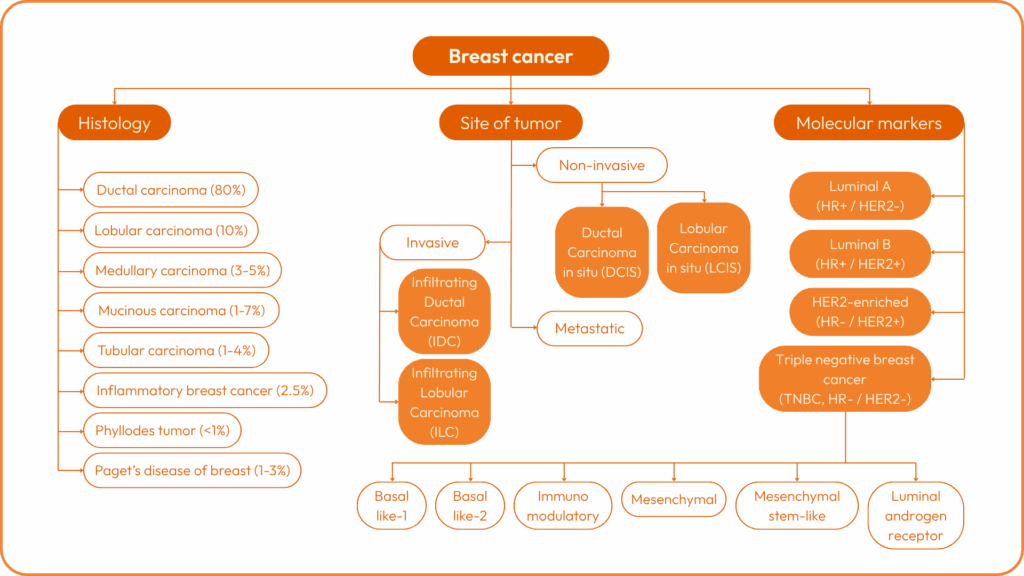
There are several types of breast cancer:
Each cancer is then characterised by a stage from I to IV, and by a grade from I to III. Stage 4 represents metastatic cancer.
Cancer subtypes can then be determined on the basis of the expression (or otherwise) of certain molecular biomarkers:


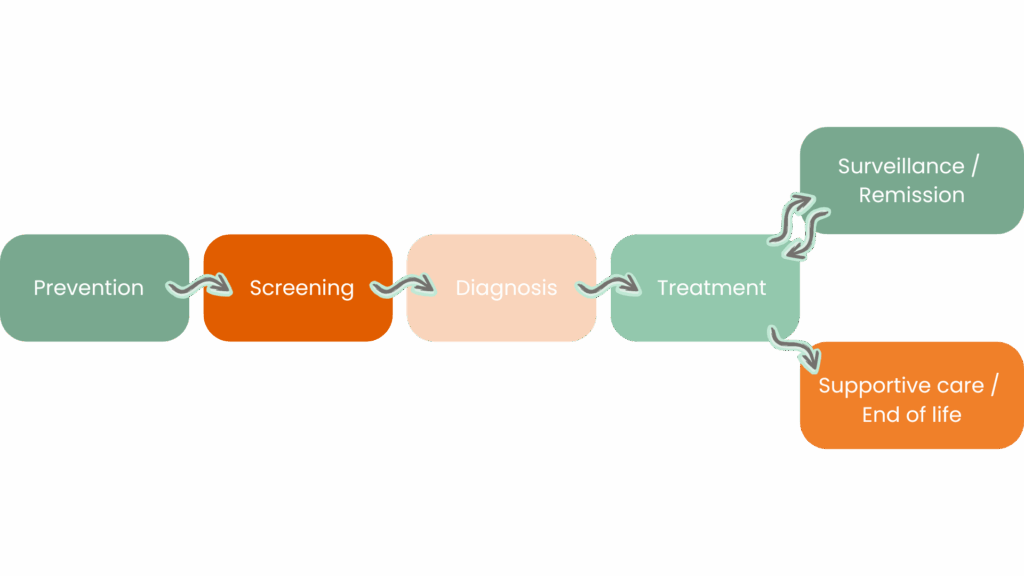
The screening phase is mainly carried out by mammography in primary care.
During the diagnostic phase, several consultations are carried out:
The diagnosis is announced on the day or within a week if the biopsy had to be taken during the initial consultation.
Once the biopsy has been taken, the work of the anatomopathology laboratory begins:
For example, HES (Haematoxylin – Eosin – Saffron) staining is used for standard diagnosis, whereas IHC (Immunohistochemistry) staining is used to identify target proteins or antigens and therefore cancer subtypes.
In our challenge, we work on IHC slides.
The staining is then carried out using a combination of machine and antibody. The choice of antibody depends on the target.
In the case of HER2, we need to :
Morgane MENARD
Head of the IMPULSE by ICO Accelerator
morgane.menard@ico.unicancer.fr
Antoine GUYONVARCH
Innovation and digital health project manager
antoine.guyonvarch@ico.unicancer.fr

